
In Ireland and the UK, Anti-vax sentiment, or vaccine hesitancy, along with deteriorating trust in the medical establishment, has set the stage for a coming plague. As a consequence of a recent outbreak of measles in the UK, Irish GP’s are now being encouraged to inform Public Health officials of suspected measles cases. The reasons for this are entirely sensible: records can be kept, cases tracked and the overall situation monitored.
Unlike COVID-19, measles is a risky disease for children, particularly immuno-suppressed ones. Few, if any, doctors dispute that it kills about one in five thousand children, and that six in a thousand will get life-threatening pneumonia or meningitis.
I don’t wish to sound alarmist; on an individual level if one of my own kids contracted measles I would not be overly concerned, but that is mainly down to them having all of the HSE-recommended childhood vaccinations (with the exception of those currently recommended for children in in respect of COVID-19).
As a result of near-universal vaccination coverage, measles presents relatively rarely in General Practice. When it is encountered in a healthy or vaccinated child, it usually causes little apprehension.
In 2017, after three years without a single recorded case in the UK, the WHO declared with great fanfare that a nation had eliminated measles. Unfortunately, Nature is not bound by WHO policy. The (somewhat deluded) party lasted for about two years, after which, cases began to re-appear; but in small enough numbers so as to be of relatively little concern in terms of public health.
Even if a single country does manage to eliminate a particular disease the absence of testing for tourists and overseas travellers makes it impossible to stamp it out completely over the long term. Viruses and bacteria don’t need passports.
Given the paucity of measles cases in Ireland – it had been years since I encountered a case – I was surprised when an email arrived from the authorities reminding me that I should report all cases to the Department of Health, and that, at the weekends, these notifications should be made through the emergency services. I was even more surprised that while working over the February bank holiday weekend to be reporting three suspected cases.
The current outbreak in the UK has yet to be declared an ‘epidemic’. I imagine there are political reasons for this reluctance; but, given the highly contagious nature of the disease and the current level of cases it is perhaps only a matter of time before that changes.
Measles is one of the most highly transmissible viruses. It is far more virulent than COVID-19 and has an infectivity rate of almost 100%. Being in the same room as a child with measles for no more than a few minutes is likely to result in transmission. Again, this is not intended as scaremongering, it is merely to point out that what is now happening in the UK is almost certainly happening in Ireland too.
According to our own HSE, COVID-19 has an infection fatality rate of 0.17 deaths per 100,000 cases (roughly one death in a million cases) in children. Measles has an infection fatality rate of 300 per 100,000 cases in children under five-years-old. The reason I trust the medical consensus on this is that measles has been the subject of research and study for decades. The same cannot be said for COVID-19.

Image Matthias Zomer.
The short unhappy life of ‘Herd-Immunity’
When a population is vaccinated against measles to a level of about 95%, the remaining 5% of unvaccinated children remain safe, as a consequence of the much-abused term, ‘herd-immunity’. This simply refers to the fact that those not immunised or vaccinated enjoy immunity by virtue of the majority of other people around them having immunity.
Immunity can come from vaccination, or from having contracted the disease. With herd immunity, measles (much like COVID-19) can’t spread as easily to those more vulnerable to the disease. This is because, even though naturally immune or vaccinated people will get the virus, their symptoms should be relatively minor. The duration of their infection should be briefer, and thus the potential spread to the vulnerable, or the 5% of unvaccinated, becomes less likely.
There comes a tipping point when vaccination or immunity levels fall below a threshold of 95%. Then herd-immunity fails and the unvaccinated and vulnerable are no longer protected. Infections become not only more common among the vaccinated, but, importantly, potentially dangerous to the unvaccinated. It is believed that in the UK for 2022-2023 the vaccination uptake (in respect of the MMR) is currently running at less than 85%. There were 1603 suspected cases of measles reported in the UK in 2023.
The current outbreak in the UK poses a number of questions, in particular: what will the consequences of a measles epidemic be in the UK and Ireland, especially for unvaccinated and immunocompromised children? As measles is presently part of an MMR vaccine, is it not reasonable to expected similar outbreaks of Mumps and Rubella?
For Measles (unlike COVID-19) there are reliable statistics going back several decades. This is research that has stood the test of time and consistent scientific review. However, after the scaremongering associated with the COVID-19 vaccination program, it is likely that many people are now sceptical about the fatality rate being talked about. Most readers will be familiar with the story of the boy who cried wolf.
In respect of morbidity and mortality the evidence in relation to measles is relatively incontestable. The risks are real, particularly for immuno-suppressed children such as those undergoing chemotherapy.
In many ways, vaccinating our own healthy kids against measles is a kind of social duty that almost all parents participate in for the greater good. It is a duty that is entirely contingent on trust in HSE vaccination advice.
After vaccination, the overwhelming majority of kids will survive a measles epidemic, however a small but significant percentage of children will suffer needlessly, and many will die.
I don’t question that there is such a thing as a vaccine injury. However, most of us take this risk and make this decision on behalf of our children, not just for their sake but, in particular, for the sake of the vulnerable. Thus, it is a reasonable expectation that all parents should shoulder some of the burden, some of the ‘risk’, and fully engage with the childhood immunisation programme.
No vaccine is ‘risk free’, sticking an empty syringe into someone’s arm comes with the very real risk of infection, cellulitis, anaphylaxis, shock etc. Indeed, no medical intervention is entirely without risk. We parents tolerate those risks because we trust the medical profession and the HSE. Throughout the pandemic, and particularly in its aftermath – where we are yet to see a formal inquiry into policies and consequences – that trust has been quite seriously eroded.

Image: Karolina Grabowska.
A question of trust?
A recent (2023) IPSOS poll found that with regards to the medical profession, surprisingly, it was the local pharmacist, and not the doctor or nurse, who topped the poll in respect of public trust.
Although fears persists over a discredited study in the late 1990s linking the MMR vaccine to autism, this was investigated and debunked. Nonetheless, damage has been done and residual hesitancy and mistrust in respect of the MMR vaccine exists to this day.
Personally and as a physician, I feel that even in the unlikely event of a tiny risk of autism associated with the MMR, I would still reluctantly have my kids vaccinated; if I thought that it would avoid death and suffering in a greater number of kids.
As stated, all vaccines come with risks that we share as parents and as a society. But that risk is contingent on trust in the medical profession, and mine has certainly been shaken in recent years.
Simple, deductive reasoning would relate the current fall in vaccine uptake to a decline of confidence in public health guidance. How has this come about?
In March/April, 2020 elderly nursing home residents were thrown under the bus, as untested hospital patients were dumped into the nursing home sector, and do not resuscitate orders (DNRs) were made. All of this carry on is now common knowledge.
Even the Zero-Covid fanatics must have raised an eyebrow at policies that linked the transmissibility of a virus to the amount of money spent in a pub. The COVID-19 vaccines were, unequivocally, forced on non-vulnerable people throughout the pandemic. The levels of coercion applied in terms of mandates and passports was absolutely unprecedented. This was reinforced by the public vilification of any individual who dared to decline or expressed fears over taking the vaccine
There were many stark warnings of censure from the regulator (IMC) for any doctor in Ireland who failed in his or her “duty to follow and promote NPHET policy.”

Image: Beyzaa Yurtkuran.
Language Games
Now that the dust has begun to settle, many people have come to recognise that the use of the word ‘vaccine’ to describe the COVID-19 jab, was (and is) problematic. COVID-19 ‘vaccines’ are, technically speaking, not vaccines in the traditional sense. They are pieces of genetic material (DNA, mRNA) that work in an entirely different manner to traditional vaccines. They are more correctly referred to as ‘gene therapy’ or ‘genetic vaccinations’ and prior to COVID-19 they had never been permitted for use in the general public.
Calling the injections ‘vaccinations’ from the outset, effectively (but rather deviously) attached this novel technology to all of the antecedent good that traditional sub-unit vaccines have accomplished throughout the centuries. Language is a powerful weapon.
As more people have had the time to look into the difference between a ‘Covid jab’ and a traditional vaccine, the ‘lie’ or at least the misappropriation of the term ‘vaccine’ has become increasingly apparent.
Two of the original four genetic vaccines (the two DNA vaccines) were quietly removed from circulation within the first few months of use. Although at the time the government declared (in an Orwellian way) that this was because they were in “short supply”. In truth, it had become clear that they were associated with significantly higher level of side effects than the mRNA type. This difference was not apparent to a frightened public during the pandemic, but more people are aware of that difference today, and that awareness is growing, in spite of the semantics.
One of the difficulties in respect of ‘the science’, ‘the facts’ or the ‘data’, during the pandemic, has been over problems with interpretation. For example: the meaning of a ‘Covid death’. Was that unfortunate death caused by COVID-19? Or was it an expected death in a very elderly person from pneumonia? Or someone who simply had a positive PCR test within the preceding two weeks? We must remember too that emergency COVID-19 funding for the nursing home sector was contingent on the reported number of COVID-19 cases.
Then there is the cycle threshold of the PCR test itself, detecting the presence of traces of the virus, as opposed to clinically relevant infections; and then plastering these dodgy ‘facts’ before a frightened public, day after day and night after night.
The overall effect of COVID-19 upon nations has invariably been described in terms of deaths per million. This metric was applied in spite of how COVID-19 mortality being overwhelmingly confined to over sixty-fives. Different countries have vastly different demographic structures, making the famous ‘deaths per million’ statistic, almost entirely irrelevant.
Many doctors tried to point these contrary facts out throughout the pandemic; all were silenced with anti-vax and even ‘right wing’ slurs. One GP was suspended and many more (including myself) were put on trial by the regulator and are awaiting sentencing. Therefore, it is important (to myself and my “anti-vax” colleagues) to unpack the accusation before we are also blamed by the regulator for the coming plague.

Image: Daniele Idini.
A nation of ‘Anti-vaxers’?
It may surprise people to learn that so far this season, between 18/9/23 and 16/01/2024, 82% of Ireland’s Healthcare Workers (including Doctors and Nurses) have NOT taken the COVID-19 vaccination booster.
If that is not bad enough, 64% of Healthcare Workers have not taken the influenza vaccine either, which is NOT a genetic vaccine. This is a truly shocking statistic as it would imply that the vast majority of healthcare workers, who are responsible for promoting and administering the COVID-19 and influenza vaccines, have not availed of either themselves.
Uptake of Autumn Booster & Seasonal Influenza doses by HSE HCWs since 18/09/2023 to 16/01/2024
In total 109,136 records for HSE HCWs were included in the analysis.
- Overall Uptake • 19,843 received COVID-19 vaccine, an uptake of 18.2%
- 39,719 received influenza vaccine, an uptake of 36.4%
The fact that myself and several of my GP colleagues are presently being prosecuted by the regulator for being critical of what purports to be a ‘vaccine’, which is currently being avoided by 82% of our colleagues, tells a story in itself, one that is very political and very Eyrish.
In the nursing home sector, where those most vulnerable to death from COVID-19 currently reside, 22% of residents have not availed of the COVID-19 vaccine and 16% have not availed of the influenza vaccine. 82% of the workers who care for them have not been vaccinated against either.
If we were living in a democracy, as opposed to a corporate-ocracy, these figures would represent a resounding vote of ‘no confidence’ in any Minister. Silence in the mainstream media clearly shows (once again) who is actually paying the piper.
Unbelievable as it may seem, the situation becomes even more bleak (or ridiculous depending on your perspective) when one considers the current public health advice in respect of COVID-19 vaccines for children. The HSE’s website as of 06/02/24 outlines the following guidance:

Irish children over the age of six months are apparently in need of vaccination: ‘to give them protection against serious Covid-19 illness.’
Despite the scaremongering, many parents are now aware that this advice is tantamount to a ‘lie’, or at the very least, a gross exaggeration. It is vanishingly rare for COVID-19 to cause “serious illness” in children.
Most people are surely wondering why this misinformation continues? If the HSE cannot be trusted in respect of the COVID-19 vaccine advice, people may also wonder whether it can be trusted in respect of other vaccines.
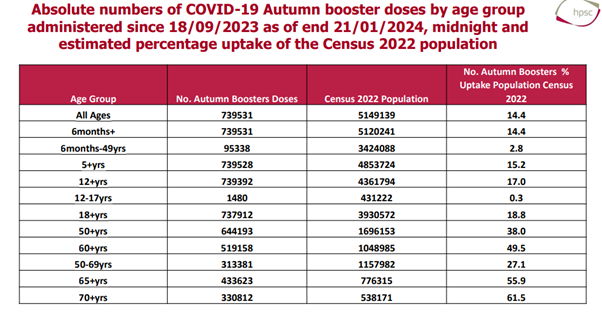
What the above (HSE) table shows is that the uptake of COVID-19 vaccination this season for people between the ages of six months and fifty years of age is 2.8%, i.e., more than 97% of people in that age category have not availed of a COVID-19 vaccines this winter, in spite of HSE advice to do so.
The numbers become even more stark when one looks at the uptake in kids between twelve and seventeen: a mere 0.3%. As these figures are derived from 2022 census data the actual uptake is likely to be even lower, as the population has increased since 2022!
The salient point is that 82% of health care workers have thus far declined the vaccine, and 97% of those under the age of fifty have also declined it, while 99.7% of the parents of twelve to seventeen year olds. All of these ‘Anti-vaxers’ have declined, despite advice from the HSE. Now what does this say in respect of confidence in the advice from the Minister or the HSE?
I sincerely hope that most people are capable of distinguishing between advice as it pertains to COVID-19 vaccines, and advice that relates to tried and trusted vaccines included in the childhood immunisation programme. There can be no doubt in anyone’s mind that this resounding national rejection of HSE guidance by members of the general public, and by an overwhelming majority of healthcare workers, reflects a lack of confidence, which is bound to have an impact on the uptake of vaccines in general.
As alluded to, in the case of measles it merely takes a fall below 90-95% uptake of vaccines before herd immunity becomes ineffective at preventing outbreaks and even epidemics.
Excess Mortality
Another contributor to the current lack of confidence in the government’s health policies has been the recent emergence of OECD mortality analysis. Unlike the equivocation that might surround data points in respect of ‘cause of death’, ‘PCR cases’ and various other data sets, there is almost no equivocation surrounding mortality figures themselves.
Sadly, when someone dies, they are dead. There is little occasion for debate, confusion or obfuscation in that regard. The number of people who die in Ireland each year is a number that cannot really be interfered with by vested interests. Whilst there might be debate about cause and diagnosis, the date and occurrence of deaths are unequivocal.
Every year in Ireland c. 55,000 babies are born and approximately 32,000 people die. The numbers fluctuate a little in line with population increases etc., but the ‘death rate’ and the ‘birth rate’ generally remain the same. If the death rate increases unexpectedly, as one would expect following a disaster of some kind, like; an earthquake, a tsunami or a pandemic for example, the increase in deaths are then referred to as ‘excess mortality.’
For almost two straight years during the COVID-19-era, the Irish people were subjected to a nightly announcement on RTE news – ‘ringing out the dead’– pointing to the catastrophic daily loss of life that was occurring across the nation. To this day the official figure in respect of COVID-19 deaths stands at almost ten thousand.
One would think that a tragedy that has resulted in so much death will naturally register in respect of our mortality figures? That there will of course be a massive increase in excess mortality during the pandemic? The straight answer here is no! It seems there was no increase in excess mortality for the years 2020, 2021 and 2022. A truth that is fully accepted and even embraced by the government!
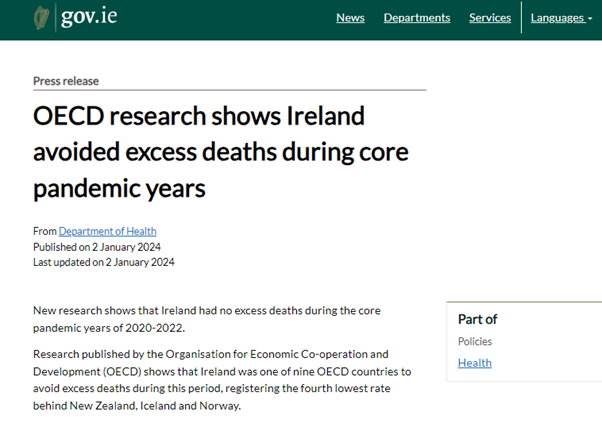
In 2023 the OECD analysed mortality figures in Ireland and elsewhere for the duration of the pandemic. They came to the conclusion that for the years 2020, 2021, and 2022 there was NO excess mortality in ireland, i.e. during the years of the pandemic there was no increase in the number of expected deaths.
An immediate reaction might be to assume that the OECD crowd are a bunch of ‘Plandemic’ conspiracy nuts! Perhaps they got something seriously wrong? Truth is that the OECD is one of the most credible sources of data on the planet. And yes, they did make all the appropriate calculations for an increase in the population due to immigration etc.
Remember, Ireland had a census in 2022, so they had the most up-to-date figures to hand. You can’t get a more accurate assessment than the OECD findings.
So where did the ten thousand COVID-19 deaths go? All of the reported deaths within the nursing home sector were real. I witnessed this myself as fourteen of my own nursing home patients died in the space of a couple of months.
Tragic as any death is, the majority in this case were part of the expected mortality in each given year, hastened by several months as a consequence of inept government policy. Most of the COVID-19 deaths that occurred outside the nursing home sector were recorded in people with a positive PCR test, as opposed to having died as a direct consequence of Covid-19.
The official figure of almost ten thousand deaths from COVID-19 represents about a third of the total deaths one would expect to see in Ireland in a given year. Those deaths must surely have affected our mortality figures in some observable way? They did not because they were part of the (tragic) but entirely ‘normal’ number of deaths that Ireland experiences each year.
What the OECD figures tell quite clearly is that if the pandemic was not a “hoax” then its effect was systematically exaggerated. A claim that in spite of the figures, remains confined to the realm of conspiracy and far from any danger of a public inquiry.
So what does the Government have to say in respect of the OECD findings? For three long years we were informed that we were enduring the worst pandemic in living memory. Policies aimed at reducing loss of life cost the exchequer thirty billion euro for the first two years. Yet there was no excess loss of life and the ten thousand ‘COVID-19 deaths’ melt into the normal yearly mortality figures?
Obviously both positions are mutually exclusive: one cannot have a pandemic with ten thousand deaths and have no increase in excess mortality.
Unfortunately for the Government there is absolutely no point in trying to deny the OECD findings. So they decided to embrace warmly, gratuitously even, their analysis, asserting that the reason there had been no excess deaths was because of the “success” of government policies throughout the pandemic. Their response is only two pages long and I would urge everyone to read it in its entirety.
It is truly frightening in terms of the paucity of credit it extends to the intelligence of the Irish people. Minister Donnelly said:
Ireland asked a lot of its population during this time and the restrictions that were put in place had a profound impact on us all.
These figures point to the success of Ireland’s public health measures, and to the strong uptake of our COVID-19 vaccination programme.
Chief Medical Officer Professor Breda Smyth said:
The OECD Working Paper highlights some of the important caveats associated with previously published estimates on excess mortality during the core pandemic years.
The population in Ireland demonstrated a strong adherence to public health measures during this time, and Ireland’s COVID-19 vaccination programme has been one of the most successful in the world, with 96% of the adult population receiving their primary vaccinations.
We know that vaccines save lives, as well as preventing serious illness and hospitalisations.
COVID is still with us, and immunity wanes over time, so I would like to remind all those who are eligible to top up their protection with a COVID booster this winter, as well as keeping up to date with their flu vaccine.
The mysterious Cheshire cat-like presence and disappearance of ten thousand COVID-19 deaths is almost magical. It (the cat) appears when the Government wishes to justify lockdowns, vaccine passports and additional billions in expenditure. But in response to the OECD findings its voice is drowned out by a cacophony of self-praise.
The disappearance of excess mortality is explained by the public’s (96%) enthusiasm for a (effectively mandatory) vaccine. But wait a minute! If there were no excess deaths in 2020, and the vaccine did not arrive in Ireland until 2021, how could the vaccine possibly account for no excess deaths in 2020?
In fact, by February 2021 at the height of ‘the second wave’ a mere ten per cent of the population had been vaccinated. I doubt whether most people in Ireland are gullible enough to believe in vanishing cats, but I could be wrong. Certainly trust in journalism appears to have plummeted to just 40% according to a recent survey.
Interestingly, in respect of the OECD findings, there has been a real increase in mortality figures yet this only arrives after the pandemic, in 2023. Myself and many others attribute this ‘spike’ in excess deaths in 2023 to the palpable consequence of missed diagnoses, closed clinics and screening programmes during the lockdowns.
{kind=link}
There is of course a growing school of thought that associates the increase in excess mortality in 2023 with side effects from the ‘vaccine’ itself. I am more sceptical on this account. However, it is a hypothesis that is difficult to dismiss out of hand.
Determining this issue is not helped by the barriers people face in trying to record a vaccine-related side-effect or death in Ireland. Beyond logging on to an obscure HPRA website and filling out a seven-page form, there is neither the observable means, nor any degree of encouragement, for doctors, or the general public, to report adverse reactions to the COVID-19 vaccines. Unlike a ‘COVID-19 death’, deaths that occurs within two weeks of a COVID-19 vaccine are not recorded as a ‘vaccine-related death’. In such cases the vaccine does not even get a mention.
The HSE are currently running a campaign informing people how to recognise a thrombosis (a recognised potential side effect of mRNA vaccines), yet there is not a single poster in a single medical office in the entire country that might explain how to record or report a side effect related to the vaccine itself.
I suspect that a growing number of people in Ireland are aware of the official misinformation in relation to COVID-19. Many of us understand that what occurred during the pandemic was based on lies and deception. The most immediate question we must attempt to answer is not whether we were lied to – that much is obvious – the real question is why? Who are the people who have profited from those lies? If we follow the chem-trails in the wake of the thirty billion euros where will this lead us?
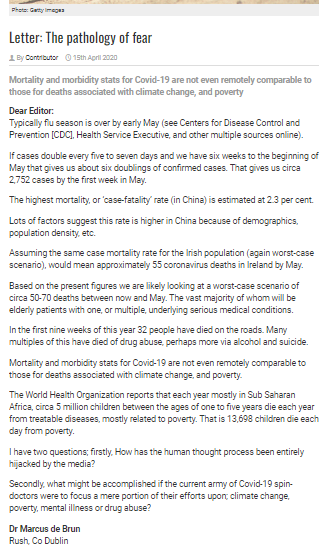
Blame the regulator
Four years ago on 15/04/2020, shortly after the arrival of COVID-19 in Ireland I published the above letter in the Irish Medical Times; a paper predominately read by Irish doctors. I tried to debunk the COVID-19 myth before it got off the ground, estimating a total of no more than fifty-five COVID-19 deaths for the first five months of 2020. It was the beginning of the end of my career in General Practice. I was pilloried and vilified[ by a small, but highly influential, clique, some of whom are the Taoiseach’s chums. The attacks were such that colleagues (with a few exceptions) who might have harboured similar suspicions, learned very quickly, to keep very quiet.
At the time a large payout for General Practice was unfolding before our eyes, beginning with a payment for each time we answered the telephone. In April, 2020, before the full extent of the neglect in the nursing homes had become apparent, I resigned from the Irish Medical Council in an attempt to highlight what was happening. My resignation was ignored by the Medical Council, who then lied to the media, saying that I had resigned for “personal reasons”.
It might seem petty to complain about the description, “for personal reasons”, but it was targeted to a specific audience of colleagues and journalists. My credibility as a doctor was being undermined. I was “not fit for purpose.” Thus, anything I might have to say on the issue of COVID-19 or nursing home deaths was tainted.
Shortly after my resignation, I was placed under investigation by the IMC and am presently awaiting a date for my fitness-to-practice hearing. One colleague Dr. Gerry Waters (a braver man than I) has already been suspended for calling the pandemic a ‘hoax’ right from the start. Myself and several others have been compelled to wait on the equivalent of a professional ‘death row’ for several years now.
I am probably somewhat biased in my conviction that the cause of professional compliance with an at times deadly and at times idiotic array of policies, lies with the regulator: the Irish Medical Council.
Numerous people complained to them throughout the pandemic about registered doctors (Holohan, Varadkar himself and many more), who were behind the policies. The Irish Medical Council answers directly to the Minister of Health. The word from the top was clearly that rebel doctors should be silenced.
At one point the head of the Irish College of General Practitioner’s was actively encouraging discrimination against those patients who had been unable or unwilling to take the vaccine. Several doctors and members of the public lodged complaints with the regulator in respect of policies and even overt discrimination, all of it was ignored:
Without exception, every single whistleblower, every single complaint in respect of medically registered policymakers, tendered to the regulator during the pandemic was completely ignored.
Should we see an inevitable rise in disease and deaths as a consequence of the current lack of confidence in HSE guidance, it is because we learned absolutely nothing from the Banking Crisis. We have not learned that crises in Ireland stem from the unfettered power of institutions, the friendship ties between those institutions; and the abject failure of regulators who are themselves in bed with those institutions.
Should there be an increase in mortality amongst our children, those deaths might not disappear quite as easily and as mysteriously as the Cheshire Cat.