
4,915. And rising. This number can only increase or, at best, stay the same. It can never go down. Of all the innovations that governments and media around the world have come up with, seemingly independently of each other, during the ongoing Covid period perhaps the most insidious is the daily running total of deaths.
I have often wondered what purpose this number serves. At a time when we are frequently told by the media and government to ‘follow the science’, what could be more unscientific than a figure which, even when nobody is dying, looms above us as a warning that danger is ever present and nothing has improved.
But take the number of people who are unemployed, a figure that has reached terrifying proportions without any sophistry or assistance from behavioural scientists. In fact, a lot of effort is expended on massaging this number downwards from the actual amount to levels more palatable for public consumption.
But imagine that we calculated the number of unemployed by concocting a total of all those who have been laid off – jobs that have died – at any time and for any duration, during the past thirteen months? Or since unemployment began, a running total of all the people who have been unemployed ever?
What function would that number serve? Might it help prevent future unemployment? Might it better inform us of the skills and training required for our workforce? Might it be useful for analysis and reporting? As Frankie Howerd used to say, “Nay, nay, and thrice nay.” I wager any civil servant who proposed such an idea would soon be on their way to early retirement, and be about as popular with politicians as a Garda on breathalyzer duty outside Leinster House.
Yet that’s exactly what we do with the running death total (and its near twin the running case total) for Covid. If the purpose of this number is to show where we currently stand amidst the ebbs and flows of the pandemic, then surely a monthly or a weekly total would do the job better. We could then, as we do with the unemployment figure, compare this month to last (or this week to last) and judge which way we’re going. Are we moving steadily forwards? Are we tumbling hopelessly backwards? You get the idea.
Why haven’t we ever had a running total of deaths from cancer, heart attacks or diabetes? If we’d started even a year ago, these numbers would be at impressive levels now. Cancer and diseases of the circulatory and respiratory systems certainly dwarf the Covid tally.
Surprisingly, Worldometer hasn’t tried to do something like this. To many of us, Worldometer is the central hub of running Covid death totals. Currently, it trumpets a formidable 593,148 deaths for the United States, a daunting 127,570 for the United Kingdom and, as mentioned at the start, a not inconsiderable 4,915 for Ireland.
But what do these frightening numbers refer to? Well, they refer to the number of Covid-19 deaths. So what’s all the fuss about? The fuss is over what constitutes a Covid-19 death. So what is meant, exactly, by a Covid-19 death? Here is where it starts to get a bit complicated.
WHO Guidance
On April 16th 2020, the World Health Organisation (WHO) issued a document entitled “International Guidelines for Certification and Classification (Coding) of Covid-19 as Cause of Death”. This provided strict rules for registration of Covid-19 deaths, rules which were fundamentally different to those which were in place for the registration of deaths from other causes.
Some doctors expressed concern about what they felt would give a misleading picture of causes of mortality. These rules, they said, were unprecedented and would lead to the over-reporting of deaths from Covid-19 and the under-reporting of deaths from other causes. Their warnings went unheeded and, for the most part, unreported. There was no place for prudence and common sense amid the frenzy and hysteria of the early days of the pandemic.
Even CMO Tony Holohan acknowledged in April last year: ‘Clinically, the “index of suspicion” for the disease would be “a good deal higher” than would normally be the case for flu.’
Covid deaths data skewed by other illnesses, says Mayo coronerhttps://t.co/2izkMNLBRF
— john burns (@JohnBurnsST) April 18, 2021
Since then numerous medical professionals have added their voices to this dissenting chorus. The latest Patrick O’ Connor is coroner for Mayo and public information officer of the Coroners Society of Ireland. O’Connor has expressed his discomfort at official reporting of Covid-19 deaths in this country: “I think numbers that are recorded as Covid deaths may be inaccurate and do not have a scientific basis”, he said earlier this month.
Let’s take a look at the International Medical Certificate of Cause of Death (MCCD). For this section I am indebted to Dr. No, the author of the ‘Bad Medicine’ blog, for his succinct explanation of how the MCCD works and how, in practice, the WHO guidelines affect this process. I recommend his article about this if you want a more detailed understanding of the topic.
The MCCD was introduced by the WHO in 1948. Its purpose was to create an international standard for the recording of deaths and to describe the sequence of events which led to a death, rather than just the immediate cause (as was common in many countries at that time).
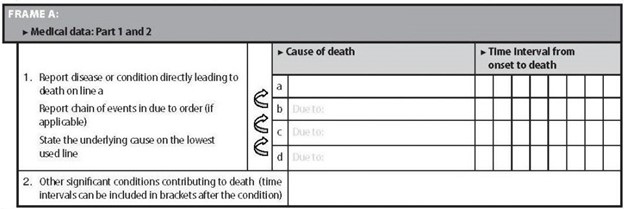
Frame A (above) is the most important part of the MCCD. It is here that all significant information about a death is recorded. As you can see, Frame A has 2 boxes. Box 1 is for recording the cause of death, Box 2 is for recording contributing conditions. Box 1, the cause of death box, has four lines: the first line records the immediate cause of death, the remaining lines record any conditions which led to the immediate cause of death, with the last line containing the underlying cause of death. The idea is to record the sequence of events which led to the death.
To give an example. A person with diabetes dies from a heart attack, which was caused by heart disease.
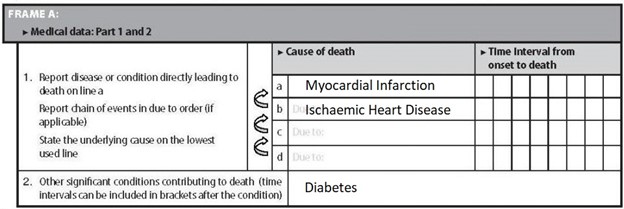
So the first line in Box 1 contains ‘Myocardial Infarction’ (the clinical name for a heart attack) because a heart attack was the immediate cause of death. The second line contains ‘Ischaemic Heart Disease’ (the clinical name for heart disease) because this is the underlying cause of death. This is the condition which initiated the sequence of events which culminated in the person’s death: the heart disease led to a heart attack. The remaining lines in Box 1 are left blank because this person had no other conditions which contributed to the sequence of events leading to their death. Diabetes is recorded in Box 2 because this is a contributing condition, rather than being a part of the sequence of events which led to death. This death will be registered as ischaemic heart disease (or simply heart disease) because this is the underlying cause of death.
Another example. A person dies from internal bleeding due to a ruptured artery as the result of a road traffic accident.
The first line in Box 1 contains ‘Internal Bleeding’ because this is the immediate cause of death.
The second line contains ‘Ruptured Artery’ because this is what led to the internal bleeding.
The third line contains ‘Road Traffic Accident’, as this was the underlying cause of death: it was a road traffic accident which initiated the sequence of events that led to the death. In this instance, Box 2 is left blank as there were no contributing conditions. So, the road traffic accident led to the ruptured artery which led to the internal bleeding. This death will be registered as a road traffic accident.
“clinically compatible illness”
The WHO’s guidelines define a Covid-19 death as “a death resulting from a clinically compatible illness, in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID disease (e.g. trauma).” This is an extremely vague definition and one which allows for a rather broad interpretation of what can be considered a Covid-19 death.
As can be seen from the HSE’s website or that of the UK’s NHS, there is a large overlap between the symptoms of Covid-19 and those of any number of other respiratory conditions or Influenza Like Illnesses (ILIs). Any of these other conditions can be considered a “clinically compatible illness”. You will note that Covid does not have to be confirmed: a “probable” case is sufficient for inclusion as a death. As Dr. No puts it, “If it looks like Covid-19, it is Covid-19.”
The guidance goes on: “A death due to COVID-19 may not be attributed to another disease (e.g. cancer) and should be counted independently of preexisting conditions that are suspected of triggering a severe course of COVID-19.” This is very important. What physicians are being told here is that, when they have identified a Covid-19 death (using the loose “if it looks like Covid” definition), then regardless of any pre-existing conditions which may have triggered severe Covid-19, the death must be registered and counted as a Covid-19 death. This goes against all conventions for identifying the cause of death.
So how does this relate to our MCCD form? Well, in our earlier examples of somebody dying from a heart attack and somebody dying in a road traffic accident, there should be no difference in the way the deaths are recorded. In fairness to the WHO, they are quite clear in their guidance that these two types of death should not be recorded as Covid-19. (Unfortunately, this has not stopped overzealous authorities around the world from registering heart failure, motor accidents, suicides and murders as Covid deaths).
However, when it comes to most other types of death, we start getting into murky waters. Take the example of a person who dies from pneumonia, caused by immobilisation, which itself was caused by multiple sclerosis.
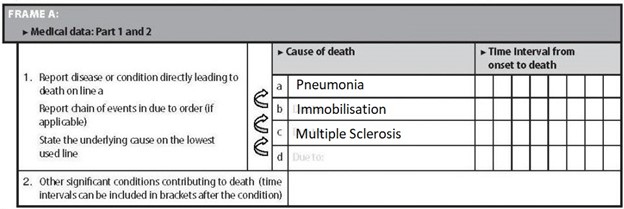
In this case, the underlying cause of death is multiple sclerosis. Why? Because multiple sclerosis led to immobilisation which led to pneumonia. So this death will be registered as multiple sclerosis.
Now, let’s imagine this person had tested positive for Covid-19.
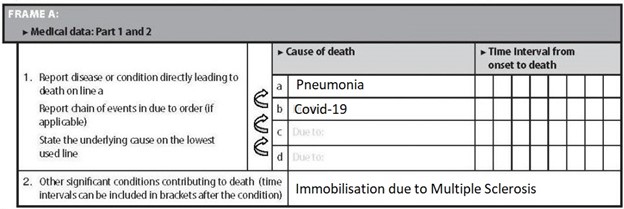
Notice anything strange? Because of the WHO guidelines, the underlying cause of death is no longer multiple sclerosis, but is instead Covid-19. Multiple sclerosis (and immobilisation) gets moved to Box 2, it’s now been relegated to a contributing condition. This death will be registered as Covid-19. Remember the WHO said in their guidelines “A death due to Covid-19 may not be attributed to another disease and should be counted independently of pre-existing conditions.”
Testing Flaws
A further issue with the above example is that the presence of Covid-19 is determined solely on the basis of a positive PCR test result. According to the WHO’s clinical coding instructions, a death must be registered as Covid-19 if the patient received a positive test result, even if they never displayed any symptoms. But PCR tests are notoriously unreliable, with even the WHO themselves warning of their tendency to produce false positive results.
@apoorva_nyc quoted the potential false positive rate at between 43% and 90% in August.
I would assume one major issue is that we are misdirecting treatment and prevention efforts from the most infectious to the non-infectious. https://t.co/LORjMJx6pu
— Michael Simonson (@msimonson19) April 30, 2021
So here we have the case of an unfortunate individual whose multiple sclerosis, over many years, caused them to become immobile. Immobility, sadly, can lead to pneumonia which, especially for the aged and/or immunocompromised, often results in death. However, because of the WHO guidance, the presence of a positive PCR result alone means that all of their medical history, the entire chain of events which led up to the person’s death, is cast aside and replaced by the misleading explanation of Covid-19.
But the issue goes even deeper. You’ll recall that the WHO’s definition of a Covid-19 death includes “probable” cases as well as “confirmed” ones. Our final example describes an individual who dies from acute respiratory distress syndrome (ARDS), caused by pneumonia, which itself was caused by chronic obstructive pulmonary disorder (COPD).
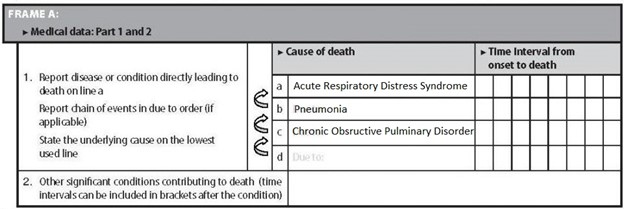
As you can see, the underlying cause of death is COPD, which led to pneumonia, which led to ARDS. This death will, of course, be registered as COPD.
But what if this person had had contact with someone known to have Covid-19 or even with a person suspected of having it? Here’s what would happen to the MCCD:
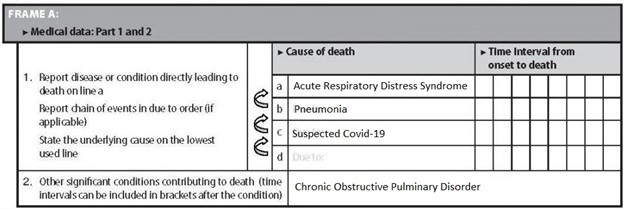
The underlying cause of death is now ‘suspected Covid-19’, which, in the figures we see on the nightly news and in the vast majority of statistics made available by governments, is treated in exactly the same way as a confirmed Covid-19 death. The WHO’s clinical coding instructions insist that it is, so long as the deceased had “contact with (a) confirmed or probable case.” The COPD which caused this person’s pneumonia is cast aside, no longer considered to have played a part in the sequence of events that led to their death.
This is absurd. Yet this is how deaths around the world are now being recorded and registered. If somebody is dying of heart disease, liver disease, respiratory disease, cancer, dementia or any other terminal illness, and they have a positive PCR test or have simply been in contact with somebody suspected of having Covid, their death is now registered and counted as a Covid-19 death. Any pre-existing condition, no matter how serious and no matter what part it played in their ultimate demise, is moved to Box 2 of the MCCD and not recorded as the underlying cause of death. The WHO guidelines state, in the section entitled “Comorbidities”, that “if the decedent had existing chronic conditions…they should be reported in Part 2 of the medical certificate of cause of death.” Conditions which for more than seventy years, since the introduction of the MCCD form, have been understood as underlying causes of death, are now rebranded as contributing factors. All to make way for the mighty Covid.
Massive Inflation
The result is a massive inflation of the numbers of Covid-19 deaths. As Patrick O’Connor, the Mayo coroner, says, when speaking about terminally ill patients, “If they prove to be Covid positive in a test, it is that (Covid) which is recorded as the principal cause of death — even though that person may have been terminally ill with a short life-expectancy prior to such testing.” And, as we have seen, a test is not even necessary, as the WHO’s guidelines instruct physicians to include “probable” with “clinically compatible” illnesses in the tallies.
Even before the WHO issued their guidelines on 16th April last year, Italian authorities had been using a similar method to register Covid deaths, with 88% of patients there (up to March 20th, 2020) having at least one comorbidity and many having two or three. In addition to hugely inflating the number of deaths from Covid-19, this bizarre way of counting also distorts the mortality rate of the disease, making it seem far more deadly than it actually is.
In 2020, a total of 73,444 people died in England and Wales with Covid-19 recorded as their underlying cause of death. In response to a freedom of information request, on 29th March 2021, the UK’s Office for National Statistics revealed that only 9,400 (12.8%) of that number were recorded without pre-existing conditions.
Interesting but not a surprise. In Ireland we counted all deaths, in all settings, suspected cases even when no lab test was done, and included people with underlying terminal illnesses who died with Covid but not of it.
— Leo Varadkar (@LeoVaradkar) July 3, 2020
On July 3rd last, Ireland’s then acting Taoiseach, Leo Varadkar, tweeted, “In Ireland we counted all deaths in all settings, suspected cases even when no lab test was done, and included people with underlying terminal illnesses who died with Covid but not of it”, revealing that the numbers of Covid-19 deaths in Ireland were vastly exaggerated and in no way reflected the lethality of the disease in this country.
Although the complete death statistics for 2020 have not yet been made available for Ireland, in April, 2021 Kildare coroner Professor Denis Cusack published a report analysing deaths in that county during the pandemic. Of 230 deaths recorded with Covid-19 as the underlying cause, 228 (99.13%) had pre-existing conditions.
Fewer than 1% Died Without a Comorbidity
I would have thought that this was a significant finding, that fewer than 1% of the people who died from Covid-19 in County Kildare did not have comorbidities. But, like anything else that doesn’t fit in with their campaign of terror against the Irish people, the Irish media was having none of it. While both RTE and The Irish Times gave coverage to Professor Cusack’s report, neither had anything to say about the 99.13% of Kildare’s Covid dead who had pre-existing medical conditions. Nor was there a mention of the average age of death in this cohort being 82.2 years of age. Both news services instead chose to focus on selected aspects of the report which they used to support the ‘lethal virus’ narrative they have long pushed. Is this censorship? Maybe it’s just extremely poor journalism.
The running total of deaths is one of the pillars that supports this whole charade. The narrative of a deadly pandemic would never have worked without the impression of huge numbers of fatalities, countless lives ‘lost to Covid’. The unprecedented changes in the way deaths are counted allowed this to happen. You would imagine such a fundamental change, one which has had such a colossal impact on every man, woman and child on the planet, would be widely reported and discussed. Yet it is almost impossible to find a mention of it anywhere in the mainstream media.
Although most of us have suffered under the heel of draconian Covid regulations, and will continue to suffer, some have profited greatly from this fiasco. We have seen how health scares have been manipulated for gain in the past, none more so than the Swine Flu pandemic that never was, in 2009, when governments, the WHO and pharmaceutical corporations colluded to profit at our expense.
There needs to be an urgent investigation, on a global scale, to find out how the Covid pantomime was allowed to happen. And we need one in Ireland, to determine who knew what and when, and exactly who has benefitted.
Walk-in Testing Centres
The current narrative being spun in Ireland is that we are close to ‘finding a way out’ of lockdown and that, if we behave ourselves, we might be permitted some limited freedoms during the summer. This is hardly surprising. We’re coming to the end of coronavirus season, which means it’s so much harder to inflate ‘cases’. And because mortality rates in the Northern Hemisphere are typically at their lowest during the summer months, it’s not as easy to attribute huge numbers of deaths to Covid-19. It was the same last summer.
But the government has been preparing for this. Already, there are 5 walk-in testing centres in operation in Ireland, with many more planned – a perfect way to boost the numbers and keep us on our toes for the summer months. And, of course, the government reserves the right, at any moment, to slap us all back into lockdown.
At the same time, it has been made abundantly clear that whatever limited freedoms we might be permitted will be contingent on mass vaccination and, before long, vaccine passports and digital identity. And don’t forget, coronavirus season comes around again in September. But, as we have seen, the lethality of this disease, for which we’ve radically changed the way we live and have forsworn so much of our freedom, has been blown out of all proportion by the fraudulent way in which deaths are registered.
We suffered under austerity for a decade. It’s hard to believe that the same politicians who decimated our health service, causing untold hardship and death, now want to protect us. Do we trust they are spending our money honestly and wisely? How much is being spent on mass vaccination, testing, tracing, the vaccine passport infrastructure? And what is the cost of the Covid period to our economy? The whole circus makes a mockery of the years of austerity and of every person who suffered because of them.
Cost to our Health
Then there is the cost to our health. Many have lost their lives because of this deception, but you don’t see a running total of their deaths on the news every night. How many have died due to a lack of primary health care, which has been sidelined and neglected, sacrificed at the altar of Covid? How many cancelled surgeries and missed screenings? What about those in urgent need of treatment who were too frightened to attend a hospital? And those who were turned away before they even reached a hospital, because Gardai at a checkpoint deemed their need not sufficiently urgent?
The mental health of our nation has taken a nosedive, not due to Covid but because of lockdowns and other unwarranted sanctions against our people. Loneliness, depression and despair have all taken their toll. The US Centres for Disease Control and Prevention (CDC), hardly a radical anti-lockdown stronghold, has estimated that one third of all excess mortality in the United States during 2020 was due to reasons other than Covid-19.
We’ve been deceived. When important facts are left out of a narrative in order to foster a misconception, we call it lying by omission. We have been lied to by politicians, public health officials, wealthy media barons and the stooges who write for them. And we have paid a terrible price. In the twilight of our freedom, it’s time for us to stand up for the truth.