
Pressing Pause
In the grip of serious illness anyone but an obtuse contrarian seeks medical assistance. As the coronavirus Covid-19 pandemic sweeps across the globe, doctors are performing heroics, often at grave risks to their own health. Enhanced screening, testing and emergency treatment facilities, along with developing a vaccine, are now paramount considerations; but we cannot ignore our underlying fragilities.
Exclusive focus on the Holy Grail of an elusive cure disregards how the virus is exploiting poverty in wealthy countries, flawed public health policies and destructive environmental practices. At least we may still soften the blow of this outbreak, and reduce the harm and incidence of future episodes. With all changed – changed utterly – returning to business-as-usual is inconceivable.
Despite what we hear from the Trump administration,[i] there are no specific medicines available to prevent or treat the new coronavirus Covid-19.[ii] The best estimate is that a year-and-a-half is the minimum time required to develop a reliable vaccine, which would actually set a record.[iii] Remarkably, a British-Italian partnership claims it will have one ready as soon as this September, but the challenge of manufacturing, distributing and mass-immunization – including the thorny issue of consent – on an unprecedented global scale, remain.[iv] The options are comprehensively laid out by medicinal chemist Derek Lowe.[v]
The dangers posed by this outbreak, and future ones that nature will throw at us, require a thorough reappraisal of public health priorities. Medical systems in advanced Western countries – especially those dominated by the private sector – tend to prioritise treatment of the symptoms of the main non-contagious diseases. We ‘live’ with cancer and heart disease as opposed to addressing multifarious lifestyle causes, which the virus is now preying on.
As Boris Johnson’s predicament underlines, anyone is susceptible to Covid-19, but chances of exposure – without recklessly ignoring medical advice – are often determined by social class, which intersects with lower life expectancy already.
"I was at a hospital the other night where I think there were actually a few coronavirus patients and I shook hands with everyone."
Boris Johnson says he has not refused to shake hands with people during the #COVID19 outbreak.
More on this story here: https://t.co/6N1ZLNKpvT pic.twitter.com/yV1qkQkDkh
— SkyNews (@SkyNews) March 3, 2020
In responding to the pandemic any nation is likely to be only as strong as its weakest links. The co-existence of extremes of poverty and wealth in societies such as the United Kingdom and U.S. poses particular dangers.
We must awaken to the environmental origins of viral diseases. What Julio Vincent Gambuto[vi] has described as this ‘Great Pause’ should bring a more harmonious relationship with nature, and other animals, as we negotiate with this and even greater environmental dangers.
Finally, as Yuval Noah Harari cogently argued:
When choosing between alternatives, we should ask ourselves not only how to overcome the immediate threat, but also what kind of world we will inhabit once the storm passes. Yes, the storm will pass, humankind will survive, most of us will still be alive — but we will inhabit a different world.[vii]
In confronting this pandemic we face a choice between top-down, authoritarian control – seen vividly in China – where basic liberties have been all-but extinguished. The alternative is a state that trusts in the collective education and responsibility of citizens – civil society – a rather extreme experiment in which is unfolding in Sweden.
There may indeed be periods when a state-imposed lockdown is justified to avert a calamity – as in Italy at the height of its surge – but we must remain vigilant to the seepage of emergency powers into ordinary usage when this crisis lifts and only countenance measures that are proportionate to risk.
Already, authoritarian regimes, such as Viktor Orban’s in Hungary,[viii] are undermining democratic institutions. Alas, the ‘Fourth Estate’ of journalism has been greatly diminished by job losses in the age of the Internet and reliance on commercial advertising, which has opened the door to regressive but digitally-savvy far-right Populism.[ix]
Social Gradient

“Nickelsville” homeless encampment, Seattle, Joe Mabel (wikicommons).
At this stage much of our knowledge of Covid-19 is provisional, but early research from the WHO in China found 78%-85% of contagions occurred in clusters within family groups.[x] Armed with knowledge of how the disease spreads and sufficient resources, affluent families around the world are taking care of elders and other vulnerable people.
However, as Charles M. Blow put it: ‘Social Distancing is a Privilege’. He reported on how incidences are highly intersected with race (which aligns with poverty in the United States), citing surveys from Milwaukee and Chicago where victims were 81 and 70 per cent African-American respectively.[xi]
Myriad factors link poverty to the contagion including: the number of residents per household; the space afforded to each occupant; the extent of inter-generational co-habitation; exposure to pollution; besides other health indicators, such as obesity. Particularly vulnerable categories include individuals squeezed into homeless shelters, or those living in crowded facilities accommodating refugees and asylum seekers; also older generations inadequately protected in residential care homes across Europe.[xii]
Notably, countries that bore the brunt of austerity policies since the Financial Crash from 2007 such as Italy, Spain, and the U.K. are now experiencing higher mortalities tolls than others, such as Germany or Denmark, where living standards were maintained.
Sweden

Swedish Social Democratic Party in Vasaparken, Stockholm in 2013, Image: Frankie Fouganthin (wikicommons)
Unlike almost every other European country the Swedish government did not mandate the closure of schools, pubs and restaurants. As the pandemic raged this seems to have been flawed, but it is worth exploring why a true catastrophe has not unfolded, as we’ve seen in Italy, Spain, France, the U.S. and the U.K.. Indeed the trajectory of new cases appears to be flattening as we enter mid-April.[xiii]
Sweden’s mortality count per capita (which is equivalent to Ireland’s whose government has generally been lauded for its response[xiv]) is four times higher than that in neighbouring Norway’s and twice Denmark’s,[xv] both of which swiftly closed their borders, schools, pubs and other businesses, and imposed lockdowns. But the divergence may, in part, be explained by recent under-investment in healthcare. The country had the second lowest number of critical beds in Europe after Portugal prior to the crisis, with only 5 beds for every 100,000 inhabitants.[xvi] Moreover, we are yet to measure the health benefits of avoiding draconian measures.
Cultural factors such as the absence of kissing and hugging as conventional greetings and sparse habitation are relevant, but it appears that Sweden’s mostly uninterrupted social democratic history throughout the twentieth century,[xvii] including free university education, insulates its population from the worst ravages.
Notably, 40% of Swedish households are single-person residences,[xviii] and, although the largest cities of Stockholm and Gothenburg have experienced a recent housing crisis with scarce supply and high prices,[xix] recent concerted action by the Social Democrat-Green coalition government has alleviated this, providing subsidies to builders and tweaking capital gains tax for house sellers to encourage turnover.[xx]
In contrast, English-speaking countries such as the United States and Britain (predicted to experience the worst outbreak in Europe[xxi]) have avoided intervention in the housing market, except at the very bottom of the social scale. But the ensuing ‘Financialization of Daily Life’[xxii] has been accompanied by the stripping away of welfare entitlements, bringing widespread homelessness and reliance on food banks. The current pandemic has been aggravated by political leaders so wedded to commercial priorities they seemed prepared to sacrifice the sick and the old.[xxiii]
Obesity

Image: Tibor Végh (wikicommons)
The damage wrought by free market ideologies may run deeper in terms of human health if we accept a link with another global pandemic: obesity. This condition is strongly associated with many of the pre-existing health problems that place a person at greater risk of death from Covid-19 infections, including hypertension and diabetes.[xxiv]
The onset of the obesity pandemic, now afflicting nearly two billion people around the globe,[xxv] has been linked to numerous developments, including the invention of high fructose corn syrup in 1967, as well as over-reliance on the motor car. But the arrival of Margaret Thatcher and Ronald Reagan into power in the 1980s is a generally overlooked factor.
As Avner Offer asserted: ‘Among affluent societies, the highest prevalence of obesity is to be found in countries most strongly committed to market-liberal policy norms.’ He argues: ‘if stress generates obesity, then welfare states protect against stress, and are likely to have lower states of obesity.’
He says: ‘it is appropriate to think of the rise of obesity as an eruption, and to look for another eruption to explain it’. He identifies this as the emergence of the New Right in the 1970s, and the market-liberal regimes that carried out economic and social programmes in the main English-speaking countries, and elsewhere.
With regard to the U.K., where obesity rates have almost tripled since 1979 when Margaret Thatcher came to power, he claims obesogenic conditions were already in place by the 1970s: car-use and television-watching were well established, and food was already cheap and plentiful; but that Thatcherism acted as a catalyst.
Heightened stress levels especially fuelled by employment uncertainties affect dietary choices: ‘Physiologically, stress leads individuals to prefer fatty and sweet foods, and frequently to consume more calories, exacerbating weight gain, especially in the form of risky abdominal fat.’[xxvi]
The link between insecurity, stress and obesity is supported by the ‘social gradient’ of obesity’: it is most prevalent among those at the bottom of the social scale, stressed out and living in crowded accommodation in so-called ‘food desserts’, lacking access to nutritious foodstuffs.
Public v Private Health
It is a misconception that increasing health expenditure in any Western society, above a certain level, will lead to a rise in life expectancy. In fact, there are rapidly diminishing returns on investment. Moreover, many treatments arrive with significant health warnings, and leave many of us susceptible to Covid-19.
Primary care, especially maternity services, paediatrics (including selective use of antibiotics and vaccination), and emergency treatment facilities, certainly minimises premature deaths. But countries in thrall to privatised healthcare tend to focus spending on medications, and other costly treatments, as opposed to preventive strategies. Thus the United States, which spends almost 18% of its GDP on healthcare (the highest level per capita in the world)[xxvii], has among the lowest life expectancies among advanced countries.[xxviii]
Rather than addressing the environmental and lifestyle triggers of the diseases of cancer and heart disease that are the leading causes of mortality (and morbidity), the United States supports a vast pharmaceutical industry that thrives off ill-health, just as its Military Industrial Complex profits from perpetual warfare.
Shockingly, in the United States a John Hopkins team calculated in 2016 that 250,000 deaths were caused by medical errors each year, making iatrogenic illness the third leading cause of death.[xxix]
All of this coheres with the 1971 Tudor Hart Inverse Care Law,[xxx] stating:
The availability of good medical care tends to vary inversely with the need for it in the population served. This inverse care law operates more completely where medical care is most exposed to market forces, and less so where such exposure is reduced. The market distribution of medical care is a primitive and historically outdated social form, and any return to it would further exaggerate the maldistribution of medical resources.
In other words, efficiency declines as expenditure increases, and the more privatised the health market the worse the outcomes.
Cancer and Heart Disease
Disconcertingly, Siddhartha Mukherjee characterises the history of cancer research as, ‘intensely competitive’, and featuring, ‘a grim, nearly athletic, determination.’[xxxi] Patient welfare, as opposed to survival, is often not to the fore, as experts compete for the next breakthrough in extending life, or finding an ever-elusive cure.
Apart from successfully discouraging smoking, we see insufficient focus and investment by national governments on preventive strategies, particularly in terms of nutrition, which often threaten vested interests. Confronting a virus that can often prove fatal for those on prolonged treatment courses should shift priorities.
Notably warnings ought to be provided when we purchase red and processed meat, which according to the WHO are ‘possible’ and ‘probable’ carcinogens respectively.[xxxii]
These foodstuffs, along with saturated animals fats and refined sugars, are also linked to heart disease, the other big killer in Western societies. The Harvard School of Public Health recommend a Mediterranean diet including: ‘high intake of olive oil, nuts, vegetables, fruits, and cereals; moderate intake of fish and poultry; low intake of dairy products, red meat, processed meats, and sweets; and wine in moderation, consumed with meals.’[xxxiii]
Urban planning should also inculcate more daily exercise by encouraging cycling and walking as opposed to motor car dominance. At least Covid-19 gives us a vision of how tranquil cities can be if motor cars are restricted.
Antibiotic Overuse

Another longstanding issue related to this pandemic is persistent overuse of antibiotics in most Western countries, as Covid-19 patients in hospitals are now at great risk of succumbing to infection by bacterial opportunists.[xxxiv]
Indirectly also, the welfare of a person’s microbiome, the collective term for the bacteria with which we enjoy a symbiotic relationship, is critical to overall health. Fundamental to the understanding of our complex relationship with the bacteria with which we coexist is the concept of amphibiosis: ‘the condition in which two life-forms create relationships that are either symbiotic or parasitic, depending on the context.’
Over the last seventy years we have progressively weakening this crucial organ, upsetting our cohabitants. Martin Blaser links bacterial impoverishment to the onset of a host of modern plagues including obesity, diabetes, heart-burn and GORD, asthma, a host of allergies, IBS and even autism.
According to Blaser the main source of the microbiome’s decline has been the invention in 1942 and subsequent over-use of antibiotics, which he likens to the development of the atom bomb. Apart from generally weakening our immune system, over-use in humans and in animal agriculture has given rise to superbugs such as MRSA that already kill thousands each year.
Antibiotics have saved millions of lives, and many surgical procedures are too dangerous to consider without them. However, over-use by doctors and dentists has surged in most Western countries to the extent that often the average twenty year old has taken almost twenty courses. Indeed, a 2016 study found that over 30% of antibiotics prescribed in the U.S. are unnecessary.[xxxv]
Generally, the fault does not lie with individual doctors. Besides patients demanding medication, they reflexively prescribe for sore throats to avoid occasionally fatal rheumatic fever, which typically occurs two or three weeks after an untreated strep infection and can be fatal. These infections are mainly viral and do not respond to antibiotics, but problematically a sore throat may already have been colonised by a strain of bacteria that is not causing the disease.
Today most bacterial infections are treated with broad-spectrum antibiotics. Martin Blaser asserts that: ‘Until doctors can readily distinguish viral from bacterial throat infections, they will always follow the safer course.’ He continues: ‘It is not profitable for companies to go to the trouble and enormous expense of developing new antibiotics.’[xxxvi]
Targeted antibiotics are only applicable in a small number of cases, and make little sense where companies are concerned with the bottom line, as opposed to the overall health of the patient, and society. A genuinely public healthcare system dictating research priorities would surely address this problem, and help confront Covid-19 and other respiratory diseases.
Another problem lies with the use of antibiotics in animal agriculture. Just as in humans, untreatable bacterial infections are emerging in farm animals and these are passing the species barrier into human populations. Often farmers utilise antibiotics not to treat disease but in order for these animals to grow more quickly. The practice of using sub-therapeutic doses is now banned in the EU but the law is difficult to enforce.
Blaser also connects over-use to the obesity pandemic as antibiotics also cause weight gain in humans. This is borne out by studies showing obese individuals to have far less of a range of bacterial strains compared to individuals of normal weight. An NHS study the Avon Longitudinal Study of Parents and Children showed that children who received antibiotics in the first six months of life were likely to have a higher body mass index.[xxxvii]
Air Quality
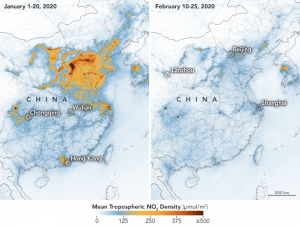
As in most crises, there is a silver lining to the Covid-19 pandemic as we witness huge improvements in air quality all across the world.
In 2008, the European Environment Agency warned that air pollution causes almost 500,000 premature deaths in Europe every year, with most of the twenty-eight EU states failing to meet air quality targets.
In 2015, about 422,000 people died prematurely in European countries from exposure to harmful levels of fine particle matter (PM2.5). These particles are too small to see or smell but cause or aggravate heart disease, asthma and lung cancer.
The report also attributed 79,000 premature deaths to the toxic gas nitrogen dioxide (NO2) – related to vehicles and central boilers. Ground-level ozone (O3) is also killing an estimated 17,700 people, prematurely, across European nations.
The main sources of air pollution are: fuel-consuming forms of transport; energy production and distribution; commercial and institutional buildings, and homes; industry agriculture, and waste management.[xxxviii]
Air pollution has been linked to elevated mortalities in hot spots such as New York and Lombardy, where the Alps are visible from Milan as never before.[xxxix] This Great Pause allows us to reflect on the necessity of much of what we produce in our economies.
Spillover

Concentrated animal feeding operation (CAFO), Unionville, Missouri, United States, owned by Smithfield Foods.
In 1994 Laurie Garrett warned the world:
While the human race battles itself, fighting over ever more crowded turf and scarcer resources, the advantage moves to the microbes’ court. They are our predators and they will be victorious if we, homo sapiens, do not learn how to live in a rational global village that affords the microbes few opportunities.[xl]
The origins of most of the contagious diseases we confront lie in our relationship with other animals. As David Quames puts it: ‘ecological disturbance causes disease to emerge. Shake a tree, and things fall out.’ He warned that human activities are causing the disintegration of ‘natural ecosystems at a cataclysmic rate.’[xli]
Correctly, a huge amount of attention has been focused on China’s so-called wet markets of captured or dead wildlife, as the probable location of a zoonotic incident that engendered the novel virus (involving bats and the rare pangolin as a reservoir host).
Previously, a southern Chinese appetite for wild animals was conflated with a period of sustained economic growth in the 1990s, and termed ’the Era of Wild Flavor.’ Businessmen would reportedly gather at one of the province’s many ‘Wild Flavor’ restaurants to feast on a great variety of animals, some of which were reputed to make consumers fan rong or ‘prosperous.’[xlii]
David Quames describes the scene at the markets:
The catfish the crabs, and eels churned slowly in aerated tanks. The bullfrogs huddled darkly in scrums. It was grim to be reminded how we doom animals with our appetite for flesh, but this place seemed no more odd or morbid than a meat market anywhere.[xliii]
He goes on to warn that the risks are not limited to exotic meat markets, and that factory and livestock farms around the world present dangers: ‘It’s almost impossible to screen your pigs, cows, chicken, ducks, sheep, and goats for a virus of any sort until you have identified that virus (or at least a close relative), and we have only begun trying. He adds: ‘tomorrow’s virus pandemic may be no more than a “blip on the productivity output” of some livestock industry today.’[xliv]
Cow fields are not a timeless and harmless rural idyll: ‘A trillion pounds of cows, fattening in feedlots and grazing on landscapes that formerly supported wild herbivores, are just another form of human impact. They are a proxy for our appetites and we are hungry.’[xlv]
Perhaps it is no coincidence that carnivorous is an anagram of coronavirus.
Little State, Big Government
Fictitious map from George Orwell’s novel 1984.
The finger must come off the pause button soon. Whether we develop a vaccine or not, we cannot indefinitely endure life as contestants on a dystopian game show. For many of us restraints on natural inclinations – including so-called ‘social distancing’ – have been traumatic. Extended lockdowns will be impossible to enforce without a descent into a barbarity of petty betrayals and transhumance; while the Chinese approach of tracking movements through smart phones – adopted in other countries too[xlvi] – is deeply sinister.
As in Sweden, civil society can adjust behavioural norms to resist this virus and others to follow, and ensure governments respond meaningfully to even more pressing challenges, such as climate change and the Sixth Extinction. We may have to accept health passports at border checkpoints for a time, but within countries, we should expect freedom to roam, interact and trade.
At this juncture we need a Little State, which does not impinge on basic liberties and privacy, but a Big Government – as in Sweden too – working to ensure conditions for human flourishing including: healthy nourishment, clean air and water, a roof over one’s head, as well as education and basic healthcare.
Anyone resistant to government intervention might consider John Rawls’s justification of a redistribution of wealth by allusion to a hypothetical rational agent, ‘situated behind a veil of ignorance.’[xlvii] This fictional character cannot know the situation he will be born into, and must decide the kind of society he would favour. If the family you are born into is a lottery, any rational person surely favours an equitable distribution of wealth.
At least we confront the prospect of another financial meltdown with an enhanced awareness of the financial clout of governments in a period of crisis. The public purse is deeper than has been acknowledged. Governments control the distribution and value ascribed to money, a measurement tool for the exchange of goods and services.
In terms of public health we can reduce the use of antibiotics and other unnecessary drugs; promote exercise and combat sedentarism; curb pollution; and highlight the danger of over-consumption of unhealthy foodstuffs.
It would be tragic if this pandemic led to the demonization and eradication of animals that could harbour suspect viruses, as opposed to leading to the permanent closure of the wet markets and hopefully factory farming too. Quite apart from the morality of this, we are dealing with highly complex ecosystems. Any measure could have unintended, dire consequences.
As the U.N.’s Sustainability Goals[xlviii] reminds us, biodiversity is essential for human flourishing. The limits of natural capital must be taken into account if economic activity is to remain sustainable, which is especially important for feeding populations. The pandemic highlights crucial interdependencies, and the catastrophic consequences of another outbreak means that the burden to adapt is shared by us all.
[i] David Smith, ‘Trump sows confusion with claim coronavirus drug will be ready soon’, The Guardian, March 19th, 2020, https://www.theguardian.com/us-news/2020/mar/19/coronavirus-drug-trump-confusion-malaria-treatment-readiness
[ii] WHO, ‘Coronavirus disease (COVID-19) advice for the public: Myth busters’ https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/myth-busters
[iii] Megan Molteni, ‘Everything You Need to Know About Coronavirus Vaccines’, Wired, April 3rd, 2020, https://www.wired.com/story/everything-you-need-to-know-about-coronavirus-vaccines/
[iv] Untitled, ‘Coronavirus: Vaccine could be ready as early as September, according to scientist’ Sky News, April 12th, 2020, https://news.sky.com/story/coronavirus-vaccine-could-be-ready-as-early-as-september-according-to-scientist-11971804
[v] Derek Lowe, ‘Coronavirus Vaccine Prospects’ In the Pipeline, April 15th, 2020 https://blogs.sciencemag.org/pipeline/
[vi] Julio Vincent Gambuto, ‘Prepare for the Ultimate Gaslighting*’, Medium April 10th, 2020, https://forge.medium.com/prepare-for-the-ultimate-gaslighting-6a8ce3f0a0e0
[vii] ‘Yuval Noah Harari: the world after coronavirus’ March 20th, 2020 https://www.ft.com/content/19d90308-6858-11ea-a3c9-1fe6fedcca75?fbclid=IwAR2am6cP4xQoG17fnKTsCeJdteQJRNwE_D6YkUkkZL25gD7AQN4CW8AOFck
[viii] Yasmen Serhan, ‘The EU Watches as Hungary Kills Democracy’, April 2nd, 2020, The Atlantic, https://www.theatlantic.com/international/archive/2020/04/europe-hungary-viktor-orban-coronavirus-covid19-democracy/609313/
[ix] Frank Armstrong, ‘Democracy in Decay: Steve Bannon & Jordan Peterson’, January 17th, 2020, Cassandra Voices, https://cassandravoices.com/current-affairs/global/democracy-in-decay-steve-bannon-and-jordan-peterson/
[x] WHO, ‘Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19)’, February, 2020, https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf
[xi] Charles M. Blow, ‘Social Distancing Is a Privilege’, New York Times, April 4th, 2020 https://www.nytimes.com/2020/04/05/opinion/coronavirus-social-distancing.html
[xii] Robert Booth, ‘Half of coronavirus deaths happen in care homes, data from EU suggests’, The Guardian, April 13th, 2020, https://www.theguardian.com/world/2020/apr/13/half-of-coronavirus-deaths-happen-in-care-homes-data-from-eu-suggests
[xiii] Worldometer, ‘Sweden’, https://www.worldometers.info/coronavirus/country/sweden/
[xiv] Frank Armstrong, ‘Ireland’s Response to the Coronavirus’, Cassandra Voices, March 28th, 2020, https://cassandravoices.com/current-affairs/irelands-response-to-the-coronavirus-pandemic/
[xv] Niclas Rolander, ‘Swedish Virus Deaths top 1000 fueling criticism over strategy’ Bloomberg, April 14th, 2020 https://www.bloomberg.com/news/articles/2020-04-14/swedish-virus-deaths-top-1-000-fueling-criticism-over-strategy
[xvi] A. Rhodes, P. Ferdinande, H. Flaatten, B. Guidet, P. G. Metnitz & R. P. Moreno, ‘The variability of critical care bed numbers in Europe’, Intensive Care Medicine volume 38, pages1647–1653(2012), https://link.springer.com/article/10.1007/s00134-012-2627-8
[xvii] Untitled, ‘Before Sweden Was Social-Democratic, An interview with Erik Bengtsson’, Jacobin Magazine, September, 2019, https://www.jacobinmag.com/2019/09/sweden-social-democracy-erik-bengtsson
[xviii] Melissa Godin, ‘Sweden’s Relaxed Approach to the Coronavirus Could Already Be Backfiring’, Time Magazine, April 9th, 2020, https://time.com/5817412/sweden-coronavirus/
[xix] Untitled, ‘Revealed: The state of Sweden’s housing shortage’, The Local, May 14th, 2019, https://www.thelocal.se/20190514/revealed-the-state-of-swedens-housing-shortage
[xx] Simon Johnson, ‘Sweden grapples with housing market reform as risks mount’, Reuters, December 18th, 2019, https://www.reuters.com/article/sweden-economy-housing/sweden-grapples-with-housing-market-reform-as-risks-mount-idUSL8N28L43A
[xxi] Rowena Mason, ‘UK could have Europe’s worst coronavirus death rate, says adviser’, April 12th, 2020, The Guardian, https://www.theguardian.com/world/2020/apr/12/uk-could-have-europes-worst-coronavirus-death-rate-says-pandemic-expert
[xxii] Randy Martin, Financialization of Daily Life, http://tupress.temple.edu/book/3182
[xxiii] Chris Smyth, ‘No 10 denies Dominic Cummings would have let elderly die’, March 23rd, 2020, The Times, https://www.thetimes.co.uk/article/no-10-denies-dominic-cummings-would-have-let-elderly-die-qsl760jr9
[xxiv] Jeffrey Kluger, ‘The True Impact of Underlying Health Conditions on Coronavirus Severity’, April 1st, 2020, Time Magazine, https://time.com/5813711/coronavirus-underlying-conditions/
[xxv] WHO, ‘Obesity and overweight’ March 3rd, 2020, https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
[xxvi] Frank Armstrong, ‘The Unbearable Heaviness of Human Beings’, October 7th, 2020, The London Magazine, https://www.thelondonmagazine.org/article/the-unbearable-heaviness-of-human-beings-2/
[xxvii] Irene Papanicolas, Liana R. Woskie, and Ashish Jha ‘Health Care Spending in the United States and Other High-Income Countries’, Commonwealth Fund, March 13th, 2018,
https://www.commonwealthfund.org/publications/journal-article/2018/mar/health-care-spending-united-states-and-other-high-income
[xxviii] OECD.stat https://stats.oecd.org/index.aspx?queryid=30114
[xxix] Vanessa McMains, ‘Johns Hopkins study suggests medical errors are third-leading cause of death in U.S.’, John Hopkins University, May 3rd, 2016, https://hub.jhu.edu/2016/05/03/medical-errors-third-leading-cause-of-death/
[xxx] Julian Tudor Hart, ‘The Inverse Care Law’, The Lancet, February 27th, 1971, https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(71)92410-X/fulltext
[xxxi] Frank Armstrong, ‘Cancer – A Distorted Version of Our Normal Selves’ Cassandra Voices, September 7th, 2019, https://cassandravoices.com/uncategorized/cancer-a-distorted-version-of-our-normal-selves/
[xxxii] Untitled, ‘Q&A on the carcinogenicity of the consumption of red meat and processed meat’, WHO October 26th, 2015 https://www.who.int/news-room/q-a-detail/q-a-on-the-carcinogenicity-of-the-consumption-of-red-meat-and-processed-meat
[xxxiii] ‘Preventing Heart Disease’, The Nutrition Source, Harvard School of Public Health, https://www.hsph.harvard.edu/nutritionsource/disease-prevention/cardiovascular-disease/preventing-cvd/
[xxxiv] Claas Kirchhelle, Adam Roberts, Andrew C. Singer, ‘Antibiotic Resistance Could Lead to More COVID-19 Deaths’, Scientific American, April 1st, 2020, 2020https://blogs.scientificamerican.com/observations/antibiotic-resistance-could-lead-to-more-covid-19-deaths/
[xxxv] Center for Disease Control and Protection, ‘CDC: 1 in 3 antibiotic prescriptions unnecessary’ https://www.cdc.gov/media/releases/2016/p0503-unnecessary-prescriptions.html
[xxxvi] Martin Blaser, Missing Microbe: How Killing Bacteria Creates Modern Plagues, One World, London 2014 pp.64-78.
[xxxvii] L. Trasande, J Blustein, M Liu, E Corwin, LM Cox, and MJ Blaser, ‘Infant antibiotic exposures and early-life body mass’ August 21st, 2012,
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3798029/
[xxxviii] Untitled, ‘Air pollution: Half a million early deaths in Europe despite progress’, BBC, October 29th, 2018, https://www.bbc.com/news/world-europe-46017339
[xxxix] Damian Carrington, ‘Air pollution linked to far higher Covid-19 death rates, study finds’ April 7th, 2020, The Guardian, https://www.theguardian.com/environment/2020/apr/07/air-pollution-linked-to-far-higher-covid-19-death-rates-study-finds?fbclid=IwAR0HF2B0LT8aNLWigzRzEhui_w1_gfndwFPP2Xfe4nvu0r2ujY78Hy56RXM
[xl] Richard Horton, ‘Coronavirus is the greatest global science policy failure in a generation’, April 7th, 2019 https://www.theguardian.com/commentisfree/2020/apr/09/deadly-virus-britain-failed-prepare-mers-sars-ebola-coronavirus
[xli] David Quames, Spillover: Animal Infections and the Next Human Pandemic, Bodley Head, London, 2012, p.23
[xlii] Cheryl Miller, ‘The Red Plague’, The New Atlantis, Winter, 2007, https://www.thenewatlantis.com/publications/the-red-plague
[xliii] Quames, p.197
[xliv] Quames, p.322
[xlv] Quames, p.497
[xlvi] Zac Doffman, ‘COVID-19 Phone Location Tracking: Yes, It’s Happening Now—Here’s What You Should Know’, Forbes, April 7th, 2020 https://www.forbes.com/sites/zakdoffman/2020/03/27/covid-19-phone-location-tracking-its-moving-fast-this-is-whats-happening-now/#1b7e565e11d3
[xlvii] Stanford Encyclopaedia of Philosophy, https://plato.stanford.edu/entries/original-position/
[xlviii] UN Sustainability Goals, https://www.un.org/sustainabledevelopment/biodiversity/