
In December 1899 Honolulu-based physicians attributed two deaths to bubonic plague, and a local paper duly announced that the ‘scourge of the Orient’ had arrived.[i] Within months a first plague fatality was reported in continental U.S. as Chinese-American Chick Gin (Wing Chung Ging or Wong Chut King depending on the transliteration) succumbed to the disease in San Francisco. The cause of death was based on a classic plague symptom of swelling around the groin, but was disputed even after rudimentary bacterial analysis. Regardless, political and health authorities were already taking actions that resonate today.
Fearing the economic impact of a dreaded disease, the state governor denied the existence of plague altogether, accusing his own health officials of propagating rumours and ‘injurious opinions’ detrimental to the ‘great and healthful city.’[ii] Conversely, successive quarantines had already been imposed on San Francisco’s Chinatown, excluding non-Asian homes and businesses despite their proximity. Enforced by barbed wire and a heavy police presence, the blockade led to dwindling food supplies and a steep rise in costs. An experimental vaccine with severe side effects, developed in 1897 by bacteriologist Waldemar Haffkine, was made obligatory for any Chinese (and Japanese) wanting to leave the city.
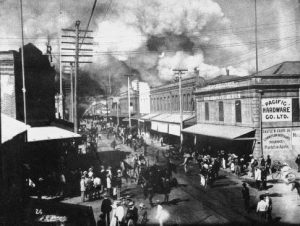
In 1900, Honolulu’s Chinatown was set on fire to in a misdirected effort to control Bubonic plague.
Unsurprisingly, the turn-of-the-century scapegoating of East Asians in California did not occur in a vacuum. Anti-Chinese prejudice had already been formalized in the Chinese Exclusion Act of 1882, banning their immigration for undermining the ‘dignity and wage scale of American workers.’[iii] There were, likewise, widespread perceptions of the Chinese as carriers of disease. If Europeans had been imperilled by the ‘barbaric hordes of Asia’, germs represented ‘a peaceful invasion more dangerous than a warlike attack.’[iv] And while dogma of the day suggested limited danger to the West due to advances in health and civilization, extreme measures might be necessary with plague. In such cases Russia’s ‘heroic methods’ in its Chinese colonies were helpfully referenced, as firing squads for the infected ‘saved trouble and other people’s lives.’[v]
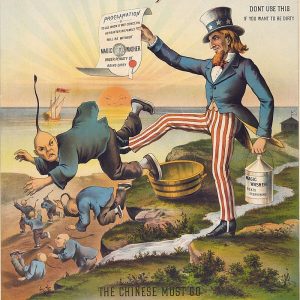
An 1886 advertisement for ‘Magic Washer’ detergent: ‘The Chinese Must Go’.
Old Wine, New Bottle
Associating disease with marginalized groups, minorities and others has hardly been an exclusively American experience. And by today’s standards, persecution over illness is not necessarily as crude, but neither can toxic discourse or indeed violence be excluded. The arrival of a new coronavirus in December 2019 is a case in point. The linking of its presumed place of origin in Wuhan with East Asians generally, and Chinese in particular, did not take long to manifest itself as multiple accounts of discrimination emerged. In Western countries this played on traditional racial tropes such as sordid animal markets and uncleanliness. Reflecting an entirely different experience, namely apprehension over Chinese influence, regional reaction was also alarmist. Both say as much about perceptions of mainland China as of the disease itself.
There is no shortage of recent examples that demonstrate medical scapegoating around a novel or poorly understood disease. In 2010, the lynching of voodoo priests in Haiti originated with rumours of pout kolera (magic cholera powder) deliberately poisoning the water supply. The choice of target was partially reflected in the complex history of voodoo practitioners and the Haitian State. At times associated with resistance to foreign occupation, at others integrated into the personality cults of Haiti’s twentieth century dictatorships, notably that of ‘Papa Doc’ Duvalier. Confusion over the origins of the cholera epidemic ‘fed on feelings of insecurity and fear’, in turn fuelling stigmatization and violence.[vi] More sustained anger eventually shifted towards the unwitting culprits, negligent United Nations peacekeepers that had contaminated the Artibonite river with cholera-infected faeces.

Vodou ceremony, Jacmel, Haiti, 2002. Image: ‘Doron’.
A corollary of medical scapegoating is fear and misinformation. Fundamental weaknesses in the Pakistani health sector, combined with accusations of a fake Hepatitis B campaign orchestrated to locate and kill Osama Bin Laden, has reinforced suspicions of polio vaccinations. With rumours of polio vaccines being either harmful or simply a front for intelligence gathering, health workers have since borne the brunt of attacks by armed groups.[vii] Misunderstandings and distortions around Ebola, both in West Africa in 2014 and more recently in the Democratic Republic of Congo have led directly to the deaths of medical staff. In the latter case, mistrust over the response is rampant, provoked in part by ‘community resentment’ over the focus on Ebola while ignoring underlying problems in the country.[viii]
The targeting of health workers as somehow responsible for bringing illness into a community, and thus the cause or at least the visible manifestation of a terrifying epidemic, is an extreme example of the need to apportion blame. But if sickness has historically been portrayed as a punishment for sin, socially excluded groups and minorities have proven most vulnerable. Whether linked to mortality or fear of the unknown, context is key to understanding the long history of how those on the margins of society have been scapegoated. Much as nineteenth century descriptions of Chinese immigrants as ‘walking time bombs of infection’ cannot be separated from pervasive Sinophobia, the frequent panic associated with novel or misunderstood illness has tended to reinforce pre-existing stereotypes.[ix]
From Tragedy to Farce
The fate of Chick Gin aside, apportioning individual responsibility for epidemics is unusual in that it is difficult to prove. ‘Typhoid Mary’ is likely the most infamous example as she came to be seen as ‘synonymous with the health menace posed by the foreign-born.’[x] An Irish immigrant cook, Mary Mallon was a so-called healthy carrier of typhoid bacteria, unintentionally instigating outbreaks amongst her wealthy employers in New York until she was eventually tracked down in 1906. Vilified in the papers as a ‘walking typhoid fever factory’ or a ‘human culture tube’,[xi] Mallon would end her days in forced isolation.

‘Typhoid’ Mary Mallon in hospital.
On a more grandiose scale, Canadian air steward Gaëtan Dugas was posthumously declared ‘Patient Zero’, accused of intentionally infecting his partners with HIV and provoking the spread of AIDS in North America.[xii] Although later disproved, the fear and exclusion of the five ‘H’s – homosexuals, heroin addicts, haemophiliacs, hookers and Haitians – remained commonplace in the 1980s.
Much like the five ‘H’s, easier to trace is the scapegoating of entire groups, the archetypal example almost certainly being the pogroms and massacres inflicted on European Jews during the Black Death. Rumours of an ‘anti-Christian international conspiracy’ fit snugly with long-standing antisemitism, particularly when mortality rates among Jews were seen as inexplicably low (the fact that sensible hygiene laws laid out in the book of Leviticus had been employed was entirely ignored). Initially directed at medieval lepers and vagrants, Jews came to be accused of poisoning wells, eventually resulting in the extermination of entire communities.[xiii] Six hundred years later hygiene control of typhus, a lice-borne pathogen, became an element of Nazi propaganda intended to justify the mass murder of human carriers during the Holocaust.[xiv]
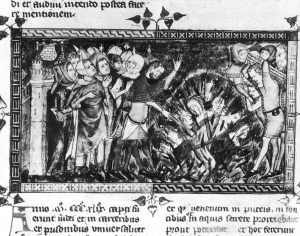
Representation of a massacre of the Jews in 1349 Antiquitates Flandriae (Royal Library of Belgium).
The transatlantic journey of yellow fever holds particular irony in the history of racial stereotyping over disease. The mosquito-borne virus’s first documented appearance in the New World was in 1647 Barbados. Even if thoroughly misunderstood at the time, much like malaria there was an assumption that black Africans were immune to the disease, all the more so as white Europeans were so highly susceptible (in reality this was largely due to early exposure during childhood). This immunity in turn became one of the justifications on which the Atlantic slave system was built. Brutal conditions on the sugar plantations and corresponding high mortality rates ensured continued new arrivals, often with the same immunity, all the while reinforcing the original racial stereotype. It was only as slavery was gradually abolished in the nineteenth century, a period coinciding with multiple outbreaks of yellow fever in the American South, that former slaves were themselves accused of spreading the disease.[xv]
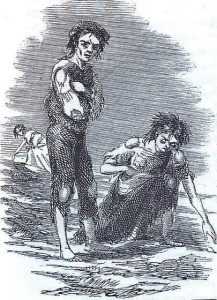
Skibbereen, west Cork, in 1847 by James Mahony.
Cholera likewise has a special place in the history of medical scapegoating and became highly politicized. Despite having long circulated locally on the Indian subcontinent, it only emerged on the global stage in the early nineteenth century, an appearance closely intertwined with colonial trade policies. As the bacteria must be ingested through contaminated water or food, the poorest and most deprived urban areas proved most vulnerable. And given the profile of its victims, the spread of cholera inevitably took on class connotations that shifted smoothly towards immigrants, even as disease transmission came to be better understood. The Irish migratory experience was strongly marked by outbreaks of cholera, with higher mortality rates used as ‘corroboration that they were carriers of the disease’ rather than a reflection of widespread discrimination and impoverishment.[xvi]
The link between poverty and disease was particularly apparent with venereal disease, more specifically syphilis (and gonorrhoea with which it was often confused). Referred to at times as the ‘secret plague’ given the strong underreporting, symptoms had been recognizable since the late fifteenth century. And while there had long been a feminized connotation as per responsibility, hence the expression ‘one night with Venus and a lifetime with Mercury’, apportioning syphilitic blame took on far more sinister connotations through the later association with underprivileged women. Various incarnations of the Contagious Diseases Act in 1860s Britain essentially allowed the arrest and forced treatment of prostitutes in an attempt to limit venereal disease in the military, and subsequently the broader population.[xvii]
The emergence of syphilis also provoked an unusual example of xenophobic scapegoating, essentially a bizarre etymological battle that took on global proportions. As the disease spread throughout Europe and beyond, rivals were duly named responsible. For the French it was the Neapolitan disease, the Italians vice versa; the Russians blamed the Poles; the Dutch turned towards the Spanish; in Japan it emerged as the ‘Chinese ulcer’; while the Turks were less discerning, simply referring to the Christian disease.[xviii] The 1918 influenza pandemic likewise went through multiple national incarnations before settling on the familiar Spanish flu, a reference to the neutral country that first reported the disease. Both examples border on the farcical and if there are lessons to be learned, at least as far as 1918 is concerned, it is rather the impact of censorship and misinformation in controlling a pandemic.[xix]
Lessons Unlearned
Being reminded of past madness has a purpose, especially as we have a nasty habit of repeating our errors. Our understandable fear of disease sadly has often revealed our basest instincts, further stigmatizing the most vulnerable and endangering the health of all. Barbaric reflexes are never far from the surface. The emergence of a new pandemic has provoked ugly reactions very much reminiscent of the past, and counterproductive to controlling both the disease and the corresponding panic. While there are no rules to the patterns of hate linked to epidemics, just as increased social cohesiveness is also a potential consequence, the choice of scapegoating targets is not random. Facile demonization of the ‘foreign’ remains a perpetual risk, and disease a convenient pretext.
As for Chick Gin, he was merely the first of many plague fatalities in 1900 San Francisco. Over the next eight years at least one-hundred-and-seventy-two others would perish, both Chinese and non-Chinese.
Duncan McLean is a senior researcher with the Research Unit on Humanitarian Stakes and Practices, Médecins Sans Frontières – Switzerland. The views expressed in this article are those of the author and in no way represent the organization to which he belongs. The content is an extension of a short editorial published in French and German, available as follows: https://www.letemps.ch/opinions/fleaux-sanitaires-aux-prejuges-sociaux; and https://www.nzz.ch/meinung/coronavirus-seuchen-suendenboecke-gesucht-ld.1543032.
[i] ‘Bubonic Plague, Breed of Filth, Here’, The Hawaiian Star, Honolulu, 12 December 1899.
[ii] ‘No Plague Says Governor Gage’, The San Francisco Call, San Francisco, 14 June 1900.
[iii] Alan M. Kraut, Silent Travelers: Germs, Genes, and the ‘Immigrant Menace’, John Hopkins University Press: Baltimore, 1994, p. 80.
[iv] ‘Chinatown is a Menace to Health’, The San Francisco Call, San Francisco, 23 November 1901.
[v] ‘The Scourge of a Century’, Lincoln County Leader, Toledo, 11 May 1900.
[vi] Ralph R. Frerichs, Deadly River: Cholera and Cover-up in Post-earthquake Haiti, Cornell University Press: Ithaca, 2016, p. 148.
[vii] ‘Winning the War on Polio in Pakistan’, International Crisis Group, Asia Report 273, 23 October 2015.
[viii] ‘DRC Ebola Outbreaks: Crisis Update’, Médecins Sans Frontières, 9 March 2020. https://www.msf.org/drc-ebola-outbreak-crisis-update
[ix] Quote taken from testimony to Congress in 1876 over the state of Chinese immigration, Mary Roberts Coolidge, Chinese Immigration, Arno Press: New York, 1969 (original 1909), p. 106.
[x] A. Kraut, see above note 3, p. 97.
[xi] ‘Woman ‘Typhoid Factory’ Held a Prisoner’, The Evening World, New York, 1 April 1907.
[xii] Charlie Campbell, Scapegoat: A History of Blaming Other People, Duckworth Overlook: London, 2011, p. 161.
[xiii] John Kelly, The Great Mortality: An intimate History of the Black Death, Harper: London, 2006, pp. 232, 248.
[xiv] Samuel K. Cohn, Pandemics: Waves of Disease, Waves of Hate from the Plague of Athens to A.I.D.S., Historical journal (Cambridge, England), 2012 November 1; 85(230): 535-555.
[xv] Sheldon Watts, Epidemics and History: Disease, Power and Imperialism, Yale University Press: London, 1999, pp. 245-246.
[xvi] Philip Alcabes, Dread: How Fear and Fantasy have Fueled Epidemics from the Black Death to Avian Flu, Public Affairs: New York, 2009, pp. 74-75, 77.
[xvii] S. Watts, see above note 15, pp. 153-54.
[xviii] Deborah Hayden, Pox: Genius, Madness, and the Mysteries of Syphilis, Basic Books: New York, 2003, p. 23.
[xix] Laura Spinney, Pale Rider: The Spanish Flu of 1918 and How it Changed the World, Jonathan Cape: London, 2017, p. 63.